
Rosa Diaz was no stranger to hunger and stress and a throbbing pain in the gut that was usually nothing serious — gastritis, she had been told, or lactose intolerance. When she became ill on the evening of Jan. 6, 2015, she figured it was the hot chocolate she’d been drinking with her family to celebrate El Día de los Reyes. It was made with milk, but she finished it anyway, savoring every drop.
In the middle of the night, her oldest daughter, Diana, found her on the couch, clutching her belly and moaning. Diana half-carried her to the bathroom, offering her some Alka-Seltzer and a sip of Gatorade to wash the antacid down. Rosa started to shiver and cry. “Let me drive you to the emergency room,” Diana urged. “No, I don’t have insurance,” Rosa protested. “I just want to go to sleep. I’m sure I’ll feel better tomorrow.”
Rosa, a 43-year-old Mexican immigrant who became a U.S. citizen in the 1990s, rarely saw doctors. She was employed through temp agencies, mostly working in factories and cleaning schools — jobs that didn’t offer insurance or pay enough to let her afford her own policy. Without realizing it, she’d become pregnant, and the fertilized egg had attached itself to her fallopian tube, instead of her uterus. The condition, an ectopic pregnancy, is extremely dangerous if not treated immediately.
Diana tucked a blanket around her mother and sat with her for a while, then went back to bed. Around 3 a.m., she heard her mother scream. Rosa’s fallopian tube had exploded, and three liters of blood — almost two-thirds of her total volume — was gushing into her abdomen. By the time paramedics delivered her to the Baylor University Medical Center emergency room in Dallas, her heart had stopped.
When Diana thinks back on the night her mother died, and what was most on her mind, she still gets angry — “because instead of wanting to feel better, she was more worried about the cost.”
From 2012 through 2015, at least 382 pregnant women and new mothers died in Texas from causes related to pregnancy and childbirth, according to the most recent data available from the Department of State Health Services; since then, hundreds more have likely perished. While their cases reflect the problems that contribute to maternal mortality across the United States — gross medical errors, deeply entrenched racism, structural deficiencies in how care is delivered — another Texas-size factor often plays a significant role: the state’s vast, and growing, problem with health insurance access.
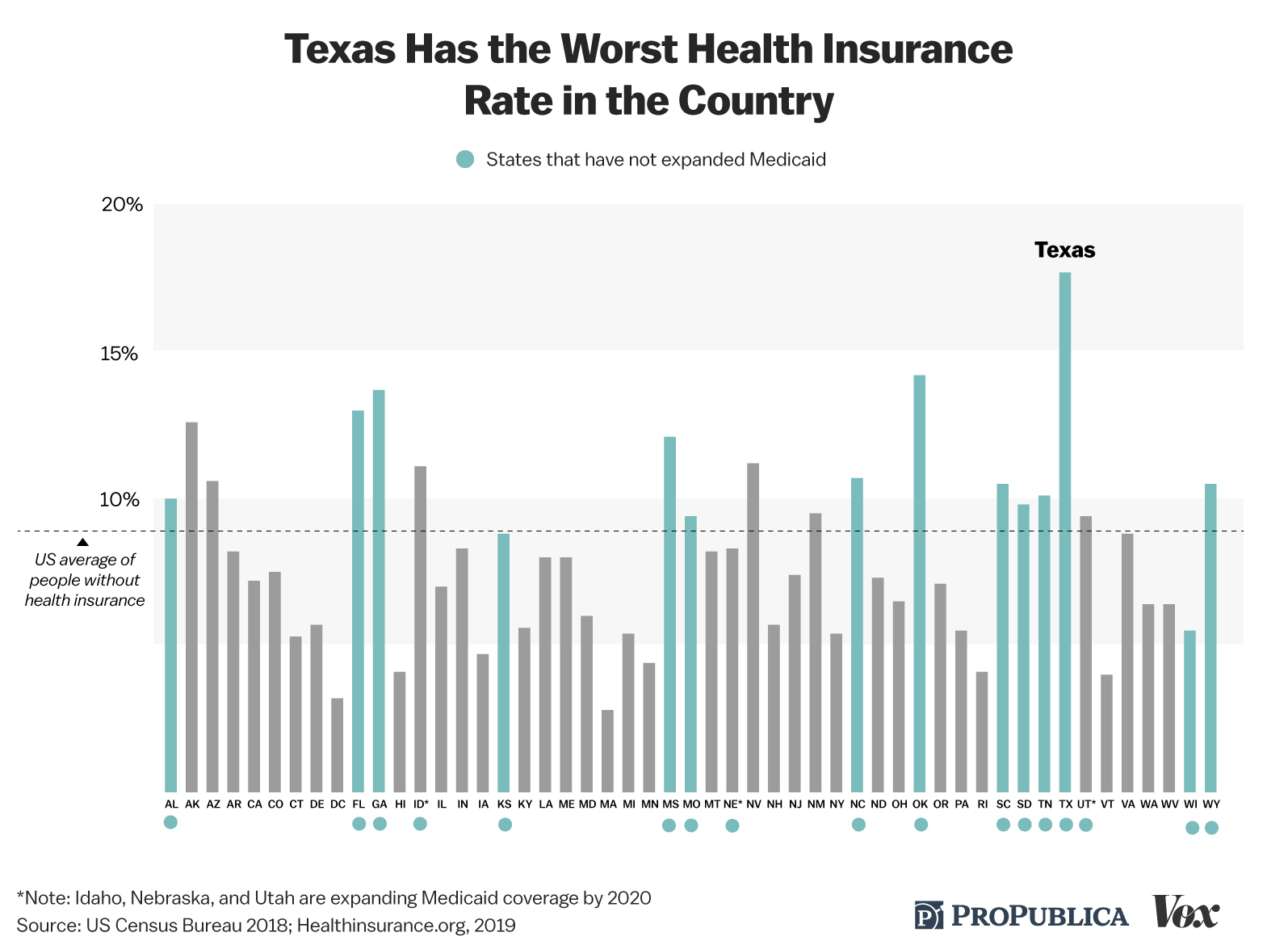
About one in six Texans — just over 5 million people — had no health insurance last year. That’s almost a sixth of all uninsured Americans, more than the entire population of neighboring Louisiana. After trending lower for several years, the Texas rate has been rising again — to 17.7% in 2018, or about twice the national average.
The numbers for women are even worse. Texas has the highest rate of uninsured women of reproductive age in the country; a third were without health coverage in 2018, according to a DSHS survey. In some counties, mainly along the Mexico border, that estimate approaches 40%.
Public health experts have long warned that such gaps can have profound consequences for women’s health across their lifespans and are a critical factor in why the U.S. has the highest rate of maternal deaths in the developed world. Texas’ maternal mortality numbers have been notably troubling, even as errors in key data have complicated efforts to understand what’s going on and led skeptics, including the governor, to question whether there’s really a crisis.
Hardly anyone outside the policy world has taken a deep look at how these insurance gaps play out for women in the second-largest state in the U.S. — at how, in the worst-case scenarios, lack of access to medical care endangers the lives of pregnant women, new mothers and babies.
ProPublica and Vox have spent the last eight months doing just that — combing through government data and reports, medical records and research studies, and talking with scores of women, health care providers, policymakers and families of lost mothers around the state. We learned about Rosa Diaz and dozens of others, mostly women of color, by scouring medical examiner’s databases for sudden, “natural” deaths, then inspecting investigator and autopsy reports for clues about what went wrong.
The picture that emerges is of a system of staggering complexity, riddled with obstacles and cracks, that prioritizes babies over mothers, thwarts women at every turn, frustrates doctors and midwives, and incentivizes substandard care. It’s “the extreme example of a fragmented system that cares about women much more in the context of delivering a healthy baby than the mother’s health in and of itself,” said Eugene Declercq, professor of community health sciences at Boston University School of Public Health.
Most of the mothers whose cases we examined were covered by Medicaid for low-income pregnant women, a state-federal health insurance program that pays for 53% of the births in Texas, more than 200,000 a year, and 43% of all births nationwide. In Texas, the program covers OB-GYN visits, medications, testing and nonobstetric care, from endocrinologists to eye exams.
But the application process is so cumbersome that women in the state have the latest entry to prenatal care in the country, ProPublica and Vox found. It can take months to be seen by regular providers and even longer to access specialists. This poses the greatest danger for high-risk mothers-to-be — as many women on Medicaid are, having had no medical care for significant parts of their lives. Then, roughly two months after delivery, pregnancy Medicaid comes to an end, and the safety net gives way to a cliff. For many new mothers, the result is a medical, emotional and financial disaster.

More than half of all maternal deaths in the U.S. now occur following delivery, according to the Centers for Disease Control and Prevention, with as many as 24% happening six or more weeks after a woman gives birth. In Texas, the proportion of late-postpartum deaths is closer to 40%, with black women bearing the greatest risk. “To lose health care coverage really has a tremendous potential to worsen outcomes,” said Dr. Lisa Hollier, chief medical officer for obstetrics and gynecology for Texas Children’s Health Plan and chair of the state’s maternal mortality review committee.
Brittney Henry’s case shows the toll. A few weeks after delivering her fourth child, the 28-year-old Houston resident suffered a heart attack, a catastrophic complication that can be associated with pregnancy. Henry went home from the hospital with a stent in her left coronary artery and a fistful of prescriptions, all paid for by pregnancy Medicaid. But after two months, those benefits lapsed and her family was left scrambling to get her the medications she needed, her husband said. On a January morning in 2016, when she was about five months postpartum, Henry begged a neighbor in her apartment complex to drive her to the emergency room. She collapsed on the sidewalk and died.
If not for her insurance struggles, her husband, Raphael Martin, asserts, the outcome might have been very different. “No bullshit,” he said, “she’d still be alive.”

A Crisis of Its Own Making
How Texas came to have the worst insurance gaps in the country is no mystery: It was an accumulation of deliberate policy choices by state lawmakers going back decades, driven largely by an aversion to government-mandated insurance and a desire to keep taxes low. “The design of our entire system is to be very limited, and historically we are very distrustful of government in general,” said Texas Rep. Sarah Davis, a Houston Republican who chairs the House Appropriations Subcommittee on Health and Human Services. Dr. Amy Raines-Milenkov, a University of North Texas Health Science Center professor and member of the state’s maternal mortality review committee, believes the state’s culture of personal responsibility leads it to abandon its most vulnerable. “We don’t have the belief here that people should have access to health care,” she said. Even the safety nets “are built on keeping people out rather than pulling people in.”
That attitude is epitomized by Texas’ approach to Medicaid. The program was established by Congress in the mid-1960s to provide access to basic medical services for the poorest of the poor; in the five decades since, it has broadened to cover 75 million Americans, many of them in the working and middle class. States have wide discretion to set income-eligibility levels for different categories of residents who receive benefits. Texas’ “traditional” Medicaid program — the one that covers nonpregnant, nondisabled adults — is the least generous in the country.
People who don’t have children or disabilities can’t receive Medicaid, no matter how poor they are. A single mother with two children only qualifies if she earns the equivalent of 17% of the federal poverty level or less — $230 to $319 per month, depending on who’s doing the calculation. That’s so little, says Anne Dunkelberg, associate director of the Center for Public Policy Priorities in Austin, that she could work 11 hours a week at a minimum wage job “and she would still make too much.” Every other state — even those more politically conservative than Texas — allows a larger portion of its residents to receive benefits. In Oklahoma, for example, the income threshold is 42% of the federal poverty level. In Tennessee, it’s 95%.
By contrast, the income threshold for pregnancy Medicaid in Texas is 12 times more generous — up to 198% of the federal poverty level, or $3,520 a month for a family of three. Under federal law, pregnancy Medicaid offers a two-month postpartum off-ramp before benefits expire. But when their coverage runs out, tens of thousands of new mothers in the state go back to being uninsured every year.

The disparity between pregnancy and traditional Medicaid is a stark measure of larger social priorities, contends Alison Stuebe, a professor of obstetrics and gynecology at the University of North Carolina School of Medicine. “If a woman’s value is 198% of the federal poverty level when she’s pregnant and 17% of the federal poverty level when she’s not, that means we’re saying a nonpregnant woman is worth 91% less than a pregnant woman.”
Eliminating such discrepancies, and improving maternal health coverage more broadly, were key goals of the Affordable Care Act. The ACA envisioned expanding Medicaid to all adults who earned up to at least 138% of the federal poverty level, regardless of whether they have children or a disability. That’s currently about $29,435 per year for a family of three. But after the U.S. Supreme Court ruled that states couldn’t be forced to accept the Medicaid expansion, Texas became one of 14 states that opted not to — a decision that has denied 1.4 million Texans of insurance who would otherwise have qualified.
Even expanding Medicaid wouldn’t address the other huge contributor to the Texas insurance crisis: Private insurance costs have also soared, and they are increasingly out of reach for everyone from Lyft drivers to public school teachers. Texans bear among the highest cost burden in the U.S. for their insurance, the Commonwealth Fund reports, spending 12% or more of their income on premiums and deductibles. Amy Beckmann, a certified nurse-midwife who splits her time between the Texas Hill Country and the Rio Grande Valley, said that she and her husband pay $1,500 a month for their medical insurance, plus a $13,000 annual family deductible: $31,000 a year. “My clients can’t afford that,” she said.
For uninsured and underinsured teenagers and women, family planning clinics like Planned Parenthood have been a crucial source of preventive care screenings as well as birth control. In 2011, Texas lawmakers gutted that system, part of a push to block abortion providers from receiving any government funding in the state. As the sweeping impacts of that decision became clear, policymakers raced to construct a new program, Healthy Texas Women, to replace some lost services. Now, the program is only serving a fraction of the women who qualify, and many doctors have stayed away, too.
A vast patchwork of other workarounds has arisen over the years to fill in the gaps left by the lack of insurance: Sliding-scale hospital systems at the county level. Free federally funded clinics. Major philanthropic initiatives and small nonprofits that subsidize everything from medications to diapers. As vital as these services are, their reach is limited, especially in rural areas, and they have the unintended effect of making the system seem even more disjointed. “The fragmentation is so huge,” Raines-Milenkov said. “On paper you can cobble services together, but in practice, you really can’t.”
And when things go wrong, when women run into an insurmountable hurdle or fall through the cracks, the sense of futility and abandonment can be overwhelming. “When you really, really, really need [help], you’re denied,” one Houston mother, Krystol Allen, said. “That makes you feel so defeated as a human being.”
The Worst for Prenatal Care

Tiffany Revilla didn’t know she was 13 weeks pregnant when she went to the emergency room in Fort Worth this past spring; all she knew was that something in her belly wasn’t right. The pain felt like a dull knife, carving her insides. As the doctor moved an ultrasound wand near one of her C-section scars, he sounded frightened: “It’s very cloudy in there. Please get help as soon as you can.”
By help, he meant an OB-GYN with the expertise to care for someone with five previous pregnancies, two preterm births, a preexisting heart condition and a uterus at high risk of rupturing or bleeding out. But Revilla’s job — the night shift at Taco Bell — didn’t come with insurance. So instead of calling a doctor, she went to McDonald’s, pulled out her phone and used the free Wi-Fi to sign up for pregnancy Medicaid.
Then, like tens of thousands of expectant mothers in Texas every year, she waited.
Texas has the worst record of first-trimester care in the country. About 21% of women who give birth in the state — some 80,000 annually — don’t see a doctor or midwife until the second trimester, according to the CDC; another one in 10 doesn’t start until the third trimester or receive any pregnancy care at all. Such delays can increase the risk of premature birth and infant mortality as well as maternal complications. In Texas, almost 11% of babies are born premature.
That’s what happened with Revilla’s fourth pregnancy in 2016. She’d barely started prenatal care at around 29 weeks when her placental sac had begun to slip out of her vagina, necessitating an emergency C-section; her son was in the neonatal intensive care unit for three and a half months. The type of incision doctors had been forced to make**,** from the top of the uterus to the bottom, put her at significant risk for future complications.
But even with her medical history and knowledge of the Medicaid system, Revilla couldn’t make the sign-up process go any faster with her most recent pregnancy. It wasn’t until she turned up at the ER again at about 18 weeks, her panties soaked in blood, suffering from what doctors feared was a placental disorder or a miscarriage, that a caseworker finally helped push through her paperwork. She didn’t have her first real prenatal appointment until 22 weeks, more than halfway through her pregnancy. Though her baby was ultimately healthy, the process Revilla had to go through to achieve that outcome was “terrible,” said her OB-GYN, Dr. Shanna Combs. “The onus is really on the patient to do everything she can to take care of her baby, yet the system doesn’t do everything that it needs to do to help her.”

The biggest driver of Texas’s prenatal delays is lack of insurance. Women can’t sign up for Medicaid until they find out they’re pregnant, and because nearly half of births are unplanned, this often doesn’t happen until the second or third month— in Revilla’s case, when she started bleeding and cramping. “I just thought it was my period,” she said. Then some women need to get their pregnancies verified by an approved provider. The Medicaid application itself is 16 times longer than a 1040 tax form. Any glitch — a forgotten document, a change of address — might cause a delay in approval or force a redo. During Revilla’s pregnancies, there were various holdups: no computer at home, applications lost in the mail, questions about why her fiance had quit his job (they’d lost their child care, so he had to stay home with the kids), difficulties getting around when he did have a job because they only had one car.
Other states have made it a priority to drastically reduce or eliminate sign-up delays. Oklahoma, where 100% of applications by pregnant women are approved instantly, verifies income after enrollment. Forty-five states and the District of Columbia consider applications within 24 hours by linking them to electronic sources, such as quarterly wage data. Texas is among the handful that still require potential enrollees to send in proof before getting care. According to a Texas Medicaid spokesperson, 92% of applicants are currently approved within 15 days. That’s “certainly progress,” said Georgetown University health policy expert Tricia Brooks, “but the vision of the ACA is to have a majority of determinations made in real time or within 24 hours.”
Even when an application is approved, simply finding a provider can present a new series of challenges. That’s largely because of another Medicaid-related problem: how little doctors and midwives are compensated.
In Texas, as in other parts of the U.S., providers are paid only about half as much for Medicaid patients as for privately insured ones. The going rate for an uncomplicated vaginal birth is about $1,500, the Texas Medical Association reports; that sum typically covers all of a patient’s normal care — a dozen or so prenatal exams, labor and delivery, and a single postpartum checkup. For a privately insured patient in Dallas, the fee is closer to $2,700, the American Medical Association says.
At the same time, Medicaid patients often are more medically and socially complex — less likely to have transportation and family support, more apt to miss appointments or be otherwise “noncompliant.” Revilla was forced to switch providers midway through an earlier pregnancy because the Medicaid-paid van she relied on was usually late and her midwife got fed up: “I kept on explaining to them that this is not my fault.”

It’s a system that many Texas OB-GYNs in private practice choose to avoid, capping the total of Medicaid patients they accept, limiting the number of high-risk women or opting out altogether. The result: more delays in initiating routine care and accessing specialists. Under Texas Medicaid rules, low-risk patients are supposed to get their first prenatal appointment within two weeks of being approved; for high-risk women, it’s supposed to be five days. But a 2016 study found much longer lag times: Only 71% of low-risk providers and 44% of high-risk ones met the state standard. Even in large urban areas like the Dallas-Fort Worth region, where Combs practices, “If I have a seizure disorder patient and I refer them to neurology, the wait time is six months.”
So the shortages lead to a vicious cycle, one that explains why prenatal care in Texas often starts so late: The harder it is for a woman to find a doctor, the later she enters care — and the harder it becomes for her to secure a doctor. Most private providers won’t take on new patients beyond the 28th week of pregnancy because of the medical and legal risks; some set the cutoff as early as 20 weeks. By then, said Dr. Erica Giwa, medical director for OB-GYN services at The Center for Children and Women in Houston, “when you see a patient … with no prenatal care, with multiple comorbidities, that looks like a ticking time bomb.”
Chronic Disease and a Lifetime Without Care
In the last few years, maternal health researchers in the U.S. have seen a dramatic shift in what kills, or nearly kills, pregnant women and new mothers. Historically, the leading medical causes were acute crises: hemorrhages, massive infections, blood clots. These days, the greatest risks come from chronic conditions diabetes, high blood pressure, heart disease that can escalate during pregnancy. According to the most recent report of the Texas maternal mortality review task force, preexisting health problems are the most common contributing factor to maternal death in the state.
These chronic diseases pose risks to women and their babies at every step of pregnancy, childbirth and the postpartum period. Women with preexisting high blood pressure, for example, are more likely to develop preeclampsia, one of the most devastating complications of pregnancy. The condition can limit the flow of nutrients to the fetus and cause the placenta to tear away from the uterus, putting the baby at risk of prematurity or death. The immediate dangers to the mother include hemorrhage, seizures and postpartum stroke — and in the longer term, heart disease.
Ideally, high blood pressure would be brought under control before a woman conceives. If that doesn’t happen, managing her hypertension during pregnancy becomes much trickier and requires careful monitoring.
More and more women in Texas need this kind of medical attention: hypertension jumped 20% in Texas women from 2005 to 2014, according to the DSHS. At the same time, prepregnancy diabetes rose 45% and obesity 25%. But even as chronic illnesses have become more prevalent, Texas’s staggeringly high uninsurance rate means many women aren’t getting treated, or even diagnosed, until they become pregnant. A few months of Medicaid, especially when prenatal care is delayed, often can’t counter years of neglect, said Dr. Sean Blackwell, the obstetrics and gynecology chair at UTHealth’s McGovern Medical School. He and his colleagues are often left “trying to prevent our train-wreck patients from having a train wreck,” he said.
The challenges multiply when women have more than one serious health problem, as 34-year-old Krystol Allen well knows.

Back when she was diagnosed with Type 2 diabetes in her late 20s, Allen was working as a teacher’s aide for special-needs kids near Houston, with decent-enough insurance to pay for her insulin and glucose test strips. But after she got married to a high school English teacher and left her job to help with a family crisis, they couldn’t afford the extra $700 a month it would have cost to cover her on his high-deductible, high-premium plan. So Allen joined the ranks of Texas’ uninsured — and quit seeing doctors and taking her meds.
By the time she found out she was expecting her older son, in 2014, she was overweight and suffering from uncontrolled high blood pressure. An extremely challenging pregnancy ended in a severe case of preeclampsia and “a really scary” emergency C-section, Allen’s OB-GYN, Giwa, recalled. Allen knew she probably wouldn’t be able to pay for her diabetes care when her pregnancy Medicaid ended. “I did not want to get pregnant again,” she said. So she opted for an IUD, a form of birth control that was supposed to last for five years.
Then Allen confronted another insurance-related problem that plagued many of the woman we spoke to for this story: difficulties with contraception. The IUD caused unbearable cramping and bleeding, so after a year and a half, she had it removed. A few months later, she was pregnant again but she hadn’t been taking her diabetes or blood pressure medications. The possibility of what that might mean for her baby made her frantic.
Poorly controlled diabetes is strongly associated with birth defects in the brain, spine and heart, miscarriage and stillbirth — especially during the critical early weeks when organs are developing. As she waited for her Medicaid to begin this time, Allen was desperate to do the right thing for her baby, whatever that might be. Finally, she and her husband went to the emergency room for advice, where a doctor told them about an option they’d never heard of: nonprescription insulin from Walmart for around $25 a vial. Allen tried it, but given her insidious combination of preexisting conditions, self-administered insulin wasn’t enough to stabilize her health. When she was finally seen by providers toward the end of her second month, Giwa recalled, “her blood sugars were terrible.”
At 22 weeks, Allen received the news she’d been dreading: an ultrasound showed that the baby had a hole in her heart. Two years later, Allen is still waiting to find out what effect the hole will have on her daughter’s long-term health or whether it will resolve naturally; doctors won’t know until the girl, Alexis, turns 3.

Uncertain about how she’ll be able to manage her health in the future, Allen recently opted to have her tubes tied. “Not only for me, but for my family, my babies,” she explained. “Being pregnant with diabetes, it could have took me out.” Meanwhile, she’s reminded every day of the implications of her untreated diabetes. Her father passed away this spring from complications of the disease after having his leg amputated, the same way her maternal grandfather died. Allen has started experiencing her own symptoms — nerve pain, blurred vision, a hangnail that took forever to heal. “What’s most scary is you’re planning for a future,” she said, “that you may not be there for.”
Just the Fetus
There is one category of patients who pose a particular conundrum for obstetric providers in Texas: immigrants. The state has the highest number of births to noncitizens outside of California, and many of those women are low-income. The large majority can’t access pregnancy Medicaid, even though most other states allow longtime legal residents to participate. Texas does have a prenatal care program for noncitizens. There’s a huge caveat, however: It doesn’t actually cover the mother, just the fetus she is carrying. It may be the ultimate example of the state’s fragmented maternal care system and how that system prioritizes babies.
The program dates back to President George W. Bush, who extended the Children’s Health Insurance Program to cover unborn babies. At the time, the idea — the fetus is a child and a future citizen and should therefore receive prenatal care — attracted more attention for its anti-abortion origins than for its potential to help immigrant mothers. In many of the 16 states that have adopted it, the type of care women receive isn’t much different than what they would get under pregnancy Medicaid.
In Texas, though, the differences are vast. CHIP Perinate provides benefits to about 33,000 women a month, regardless of their immigration status, up to 202% of the federal poverty level. But the program’s narrow focus on the fetus ignores critical aspects of a mother’s care, doctors complain, treating her “like she’s the carrier for the baby,” as Giwa put it — or “a vessel,” as Raines-Milenkov said.
For example, CHIP Perinate only covers labor if the result is an actual delivery (the cost is usually borne by another program, emergency Medicaid). Premature or “false” labor — when the mother goes to the hospital with contractions that turn out to be nothing — isn’t covered. Nor does CHIP pay for a mother’s nonobstetric emergencies, like a rotten tooth in danger of turning septic or hospitalization for a serious illness.
The gap extends to care for cardiac conditions, the leading cause of maternal death in Texas and across the U.S. “If a woman has a history of high blood pressure or diabetes, there could already be heart damage,” said Tania Lopez, a certified nurse-midwife at the JPS Health Network’s high-risk OB-GYN clinic in Fort Worth. One way to check is a maternal echocardiogram, a sonogram of the heart that private insurance and Medicaid would cover — but not CHIP Perinate, Lopez and numerous other providers said.
Read More

Some of the program’s biggest limitations come after the baby has been delivered. While new mothers get two routine checkups, those whose needs are not routine must fend for themselves. “Post-delivery services or complications resulting in the need for emergency services for the mother of the perinate are not a covered benefit,” Christine Mann, a spokesperson for the Texas Health and Human Services Commission, which administers the program, confirmed. Even life-threatening postpartum conditions like preeclampsia or blood clots are excluded under the program’s rules, though a woman might be able to get coverage under emergency Medicaid, Mann said.
The greatest postpartum need is for mental health services and contraception, according to numerous providers, neither of which CHIP covers. In Shanna Combs’ practice, it is not uncommon for CHIP Perinate patients who don’t want any more children to beg her for an unnecessary C-section, so she can do a tubal ligation at the same time, an approach that turns what would otherwise be an unaffordable sterilization into “just a small add-on cost,” Combs said.
For George Saade, chief of obstetrics and maternal fetal medicine at the University of Texas Medical Branch in Galveston, the cancer patients stand out. He recalled a case in which a CHIP Perinate patient was diagnosed with breast cancer while pregnant. She needed surgery and chemotherapy. “We had a difficult time finding care for the breast cancer,” he said, “because it wasn’t the baby and [CHIP] only covers the baby.” Eventually, “we found a place that was willing to take care of her. But that’s not ideal. That’s not the way it should work.”
The health system Saade works for will absorb some costs that CHIP Perinate won’t reimburse; other clinics said they often do the same. But many private providers said they simply refuse to deal with CHIP Perinate patients at all.
Perinatal CHIP is better than nothing, Saade said. But “the fetus can’t exist or survive without the mother being healthy. … It puts us in untenable situations, because we are, as physicians, obligated to give the patient full care, not just care for the baby.”
The Postpartum Cliff
Despite how complicated her pregnancy had been, Tiffany Revilla’s C-section this October at 37 weeks went smoothly. Back at home, though, she was in excruciating pain and so nauseated and debilitated that she could barely eat or sleep or take care of her newborn daughter. Another trip to the ER confirmed the source of her agony: multiple gallstones, including one the diameter of a large coin. Pregnancy can wreak havoc on the gallbladder, and Revilla’s pregnancy had done just that.
Revilla’s doctors worried that the stones could cause blockages and ultimately a serious infection. Removing her gallbladder so soon after her C-section “was not the perfect situation,” her OB-GYN, Combs, said. “In the ideal world, if we could space them out, we would.” But Revilla was also facing the Medicaid deadline so many women in Texas stare down after giving birth: Her benefits would expire two months postpartum. Her doctors scrambled to squeeze in her surgery. “My insides are not even healed yet,” Revilla lamented. “I don’t know how my body’s going to react. It’s very scary.”

To understand why women like Revilla are dropped off pregnancy Medicaid so soon, it helps to know the history of the program. It was a 1980s infant mortality crisis, not concern about mothers’ health, that turned pregnancy into a mandatory coverage category for states. With research aimed largely at improving outcomes for babies, 60 days of postpartum coverage seemed adequate to address a woman’s health needs. Four decades later, for most women in the U.S. regardless of their insurance status, postpartum care still amounts to a single checkup at four to six weeks after delivery.
But the scientific understanding of pregnancy and postpartum has changed fundamentally in the past few years. The three months after birth are now recognized as a critical time in the health of mothers and infants, complete with a new name: the fourth trimester. Even normal healing from childbirth can be a lengthy process, researchers are finding. Some of the most dangerous pregnancy-related complications, including preeclampsia, blood clots and heart problems such as cardiomyopathy, may not surface until weeks or months after delivery. Depression, substance-use disorders and heart conditions — three of the leading postpartum causes of maternal mortality in Texas and across the U.S. — often worsen under the economic and social stresses of new motherhood.
Instead of being a typical benchmark for recovery, the two-month mark can be “a tipping point … on the margin between illness and wellness,” said Neel Shah, an OB-GYN and assistant professor of obstetrics, gynecology and reproductive biology at Harvard Medical School. “That’s when you’re getting the least amount of sleep, you’re feeling the most socially isolated. Adding a gap in insurance on top of that not only seems that it’s in the wrong direction, but it’s also cruel.”
Medicaid benefits expire even for women who suffer health complications, like Revilla’s gallstones, that are directly related to their pregnancies or deliveries. Pregnancy Medicaid can’t be extended under any circumstances; instead, as coverage ends, women are assessed “to determine eligibility for our other products,” such as traditional or disability Medicaid, said Mann, the agency’s spokesperson. Low-income new mothers who don’t qualify for Medicaid are automatically enrolled in the Healthy Texas Women program, she added. But many women told us that in practice, the end of pregnancy Medicaid results in insurance freefall.
The urgent need to fix the gaps in postpartum care has captured the attention of national reformers, who see it as a critical step toward narrowing racial disparities in maternal mortality. Several 2020 Democratic presidential candidates have proposed federal legislation to extend pregnancy Medicaid to a full year postpartum, and state lawmakers have introduced a wave of similar bills. Missouri passed a limited extension last year and Illinois a far more sweeping one this past July; both plans are awaiting federal approval.

The enthusiasm extended to Texas, where a broad coalition, led by the maternal mortality review task force, came together this past legislative session to support a full-year extension. The effort passed the House but stalled in the Senate. “All the oxygen in the room this session was taken up by school finance reform,” the legislative priority of the state’s top Republicans, said Tim Schauer, an Austin-based lobbyist on women’s health issues. The five-year cost of extending postpartum coverage was estimated at nearly $1 billion in state and federal funds, according to Politico. Rep. Shawn Thierry, D-Houston, who introduced one of the extension bills, had to counter skeptics who thought that the state’s alarming maternal mortality numbers were, as she said, “kind of a hoax” and that increasing benefits for new mothers was just a stealth tactic aimed at expanding Medicaid more widely.
It’s an attitude Thierry’s Republican colleague, Rep. Sarah Davis, has also had to contend with. “Medicaid expansion — that’s like a four letter word [here],” Davis said. For a lot of Republicans who dominate the Statehouse, women’s health issues trigger a similar reaction, she added: “Women’s health has become so synonymous with Planned Parenthood, that in an effort to sort of punish Planned Parenthood, women in general get punished. Thus, when Davis and her Senate allies managed to pass legislation in 2017 mandating one year of postpartum depression screening for new mothers, she used the strategy she knew would work best: focusing on the baby. The benefit is part of children’s Medicaid and mothers are screened by their kids’ pediatricians. “I think [framing the issue this way] did make that more palatable to people,” Davis said.
The Texas governor’s office declined to comment for this story. Mann said in an emailed statement, “Texas is working toward better health outcomes for women, mothers and babies by offering an array of services and initiatives to help women live healthier lives and build strong families.” The state’s 2020 business plan includes worthy goals, such as expanding access to long-acting contraceptives and prenatal care. But instead of changing policy, it aims to achieve them through a series of “deliverables,” like developing informational materials and plans for reducing barriers to access.
In the absence of broader policy change, women and families find their own stopgaps, doing what they have to do to get by. Several of the dozens of women we spoke with for this story had a secret they were too ashamed, or afraid, to reveal on the record, but felt compelled to share nonetheless. One mother with Type 2 diabetes rationed insulin while pregnant, endangering her baby’s health, just so she’d have medicine left over when her Medicaid ran out. Another was in danger of going blind after being diagnosed with a pituitary tumor brought on by pregnancy hormones. She begged Medicaid officials for an extension: “I said, ‘I’m losing my eyesight.’ … And they told me, ‘Well, there’s nothing we can do.’”
Her solution: lying about where she lived, signing up for indigent care in a neighboring county and hoping she didn’t get caught. “When the card arrived, I said, ‘Thank you, Jesus.’ That was the best news I’ve had in a very long time.”
















