More than 6.5 million Americans have peripheral artery disease, a condition in which arteries are obstructed, restricting blood flow, most often in the legs. The first sign is often leg pain during activity, also known as claudication. While most treatments are safe, in recent years, experts have warned that some doctors may be subjecting patients to invasive procedures too early in their disease progression, needlessly exposing them to risks of complications, including amputation and even death.
Over the past year, ProPublica has investigated these vascular treatments, and we found some doctors are earning millions of dollars conducting a questionable number of procedures. For treatments in outpatient clinics, federal insurers, like Medicare, pay generous reimbursements to doctors, who can charge tens of thousands of dollars for procedures done in a single office visit.
Treatments include widening the arteries with stents and balloons and clearing plaque from vessel walls with a laser or bladed catheter, also known as an atherectomy. Despite minimal evidence to support the treatment’s benefits compared with less expensive alternatives, atherectomies have surged in recent years, researchers have found, with hundreds of outlier doctors performing the procedure in a majority of their patient cases.
ProPublica found that, from 2017 through 2021, about 200 doctors accounted for more than half of atherectomy procedures and Medicare payments, totaling nearly $1.5 billion, according to public federal data. Many of these physicians work in outpatient clinics.
To better understand how doctors are using the procedure, ProPublica sought to analyze Medicare data for patients who underwent atherectomy treatments, working with the data journalism team at CareSet, a health analytics group that exists to transform Medicare data into insights for better patient care.
For our analysis, we set out to understand how often doctors were performing atherectomy procedures for patients in the early stages of disease. We relied on Medicare fee-for-service claims data and examined atherectomy procedures conducted over the past four years, from 2019 through 2022, limiting our analysis to the first-time atherectomy procedures that patients underwent during this time. We focused on initial atherectomy procedures to better understand whether interventions were occuring in the early stages of vascular disease, before possible progression of the illness. For each doctor, we calculated what percentage of their patients receiving a first-time atherectomy appeared to have had only more mild vascular disease, based on a diagnosis of claudication.
What Data Was Used for the Analysis?
When a patient is treated by a physician, medical details on their diagnoses and procedures are submitted to insurers for reimbursement payments. The Centers for Medicare and Medicaid Services collect this data for patients covered by its federal insurance and share it with the public and researchers, removing names and other private information to protect patient privacy.
To examine doctor reimbursement for atherectomy procedures, ProPublica relied on Medicare’s provider use and payment dataset, which contains details on the services and procedures provided to Medicare beneficiaries by physicians and other health care professionals. This public data let us calculate how much Medicare paid each provider in reimbursement per type of procedure. We looked at five years of data, from 2017 through 2021, the most recent year available.
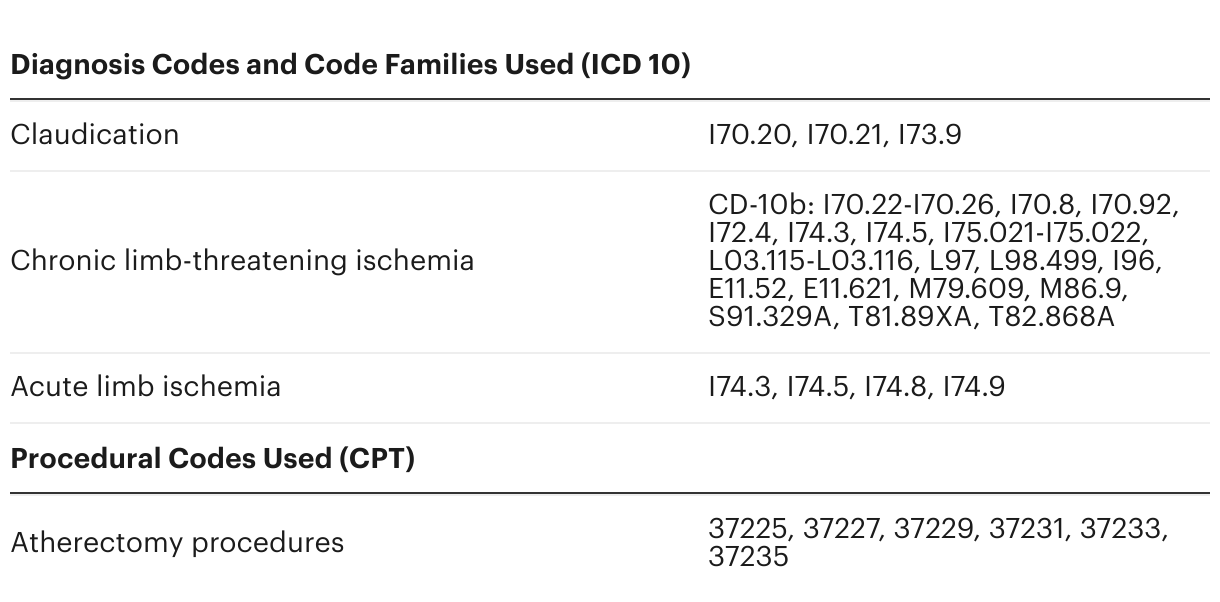
But the public reimbursement data does not include detailed information on provider behavior or patient diagnosis, so ProPublica partnered with CareSet, which has special access to Medicare claims data. The data included carrier, institutional inpatient and institutional outpatient claims. We used codes from the Current Procedural Terminology system, devised by the American Medical Association and used by Medicare, and we identified patients who underwent a first-time atherectomy procedure. We limited our analysis to patients who had procedures from Jan. 1, 2019, through Dec. 31, 2022.
We classified patients into two categories: those with more severe chronic disease, who had a diagnosis of chronic limb-threatening ischemia; and those who appeared to have milder vascular disease, based on a diagnosis of claudication. Patients with claudication were defined by the International Classification of Diseases code families I70.20, I70.21 and I73.9, a set of diagnosis codes used by other researchers in peer-reviewed studies. We omitted patients who underwent an atherectomy procedure before their first treatment in our study period. To do this, we looked back at the data 12 months before the start of our study period. We also excluded patients with a diagnosis of acute limb ischemia, which is often linked to an emergency event. We included patients who initially had a claudication diagnosis at the time of their first atherectomy procedure but whose disease may have advanced to a more severe stage during our study period, because of concerns that the interventions may have contributed to disease progression.
We pooled the patient-level data by doctor to calculate what percentage of each physician’s patients underwent a first-time atherectomy for claudication versus chronic limb-threatening ischemia.
Why Did We Focus on Patients With Claudication?
We wanted to know whether doctors who conduct atherectomies are using the procedure excessively on patients who appear to have milder vascular disease.
For many patients with peripheral artery disease, an initial symptom is pain when walking or exercising, which is also known as intermittent claudication. The discomfort often arises from limited oxygen in the leg muscles due to the narrowing of arteries, which can progressively become obstructed with plaque. According to experts, the majority of patients who experience claudication will not develop severe vascular disease, like chronic limb-threatening ischemia. While endovascular interventions are recognized by experts as appropriate for severe disease, best practices recommend that milder symptoms initially be managed by noninvasive care, which can slow or even reverse symptoms. These treatments may include exercise, diet changes, quitting smoking and medication.
The medical guidelines of several professional societies encourage starting with these noninvasive approaches. Last year, the Society for Vascular Surgery published appropriate use criteria for patients with claudication and recommended first-line treatments of exercise before resorting to interventions. It also advised against conducting procedures on arteries below the knee, emphasizing that interventions in these vessels for patients with claudication are of “unclear benefit and could be harmful.”
Just last month, the European Society for Vascular Surgery published its clinical practice guidelines on treating patients with asymptomatic peripheral artery disease and intermittent claudication, recommending conservative care for most of these patients. It also explicitly discouraged the routine use of atherectomy for patients with disabling claudication “due to the lack of superiority of atherectomy over conventional endovascular therapies in terms of efficacy and safety endpoints.”
Numerous studies have questioned the efficacy of atherectomy over the years, including from Cochrane, a widely respected network of experts that conducts systematic reviews of research. A Cochrane review found atherectomies are not necessarily more effective than alternative procedures. The studies on the effectiveness of atherectomy, it found, were small and had inconsistent results, and their methodologies had a “high risk of bias.”
While most doctors follow best practices, ProPublica has found that some opt for overly aggressive invasive treatments in early stages of vascular disease, which research has found may be associated with an increased risk of complications. In response to recent research, interviews with doctors and patients, and the recent medical guidelines and criteria, we sought to better understand doctor behavior in treating patients with claudication.
How Did We Develop Our Methodology?
Over the past year, our reporting has relied on numerous interviews with researchers, doctors and medical experts from various specialties, including but not limited to vascular surgery, interventional radiology and interventional cardiology. These conversations with experts have helped inform our analysis process. We also used several studies as a starting point for our own methodology, including some from Dr. Caitlin Hicks, an associate professor of surgery at Johns Hopkins University School of Medicine and a leading researcher on procedure overuse.
One of the principal studies we relied on was “Use of Atherectomy during Index Peripheral Vascular Interventions,” which examined first-time vascular procedures, comparing atherectomies with other endovascular interventions, such as angioplasty and stenting. The researchers found substantial variation in how doctors use atherectomies as first-time procedures, with some using the treatment sparingly and others deploying it in a majority of their cases. High rates of atherectomy were more strongly associated with patients who had claudication and for procedures conducted in outpatient settings.
Another study that informed our process was “Overuse of early peripheral vascular interventions for claudication,” which sought to understand whether physicians were adhering to best practices for treating claudication, which recommend noninvasive approaches for patients in the early stages of the disease. Most doctors follow the practice guidelines, but researchers found a group of outlier physicians with high rates of intervention in patients newly diagnosed with claudication. Doctors who worked in high-volume outpatient settings also tended to have a higher rate of early intervention, which “supports the concern that some procedures for claudication may be overused for financial gain,” the authors concluded.
We also were informed by “Practice Patterns of Vascular Surgery’s ‘1%,’” which examined the use of procedures by vascular surgeons who accounted for the top 1% of all Medicare payments. The analysis found that of the $589 million in Medicare payments that went to vascular surgeons in 2016, the top 1% of that workforce — 31 doctors — received $91 million, or 15% of all payments. These outliers also accounted for 49% of the atherectomy payments to vascular surgeons. “The dramatic differences in practice patterns raise concern for potential overuse of specific, highly reimbursed services,” the researchers wrote.
While these studies, and several others, helped inform our process, our analysis with CareSet was independently conducted and did not rely on data of other researchers. Compared with the other studies, our analysis looked at a longer time frame, four years of data, and examined a different metric, percentage of a physician’s patients with claudication at the point of their initial atherectomy procedure.
What Are Our Top-Line Findings?
Relying on public Medicare data, we found that a small fraction of physicians conducting atherectomies account for a majority of the nation’s procedures and Medicare reimbursement payments. About 200 doctors were responsible for conducting nearly 200,000 atherectomies over five years.
Even though these providers only make up about a tenth of all doctors conducting the procedure, they accounted for 53% of all atherectomies in the country. Over five years, they received nearly $1.5 billion in reimbursements for them, representing almost two-thirds of all Medicare payments for the procedures. These physicians may be conducting more procedures and receiving more payments from commercial insurance and Medicaid, as our analysis only looked at Medicare data.
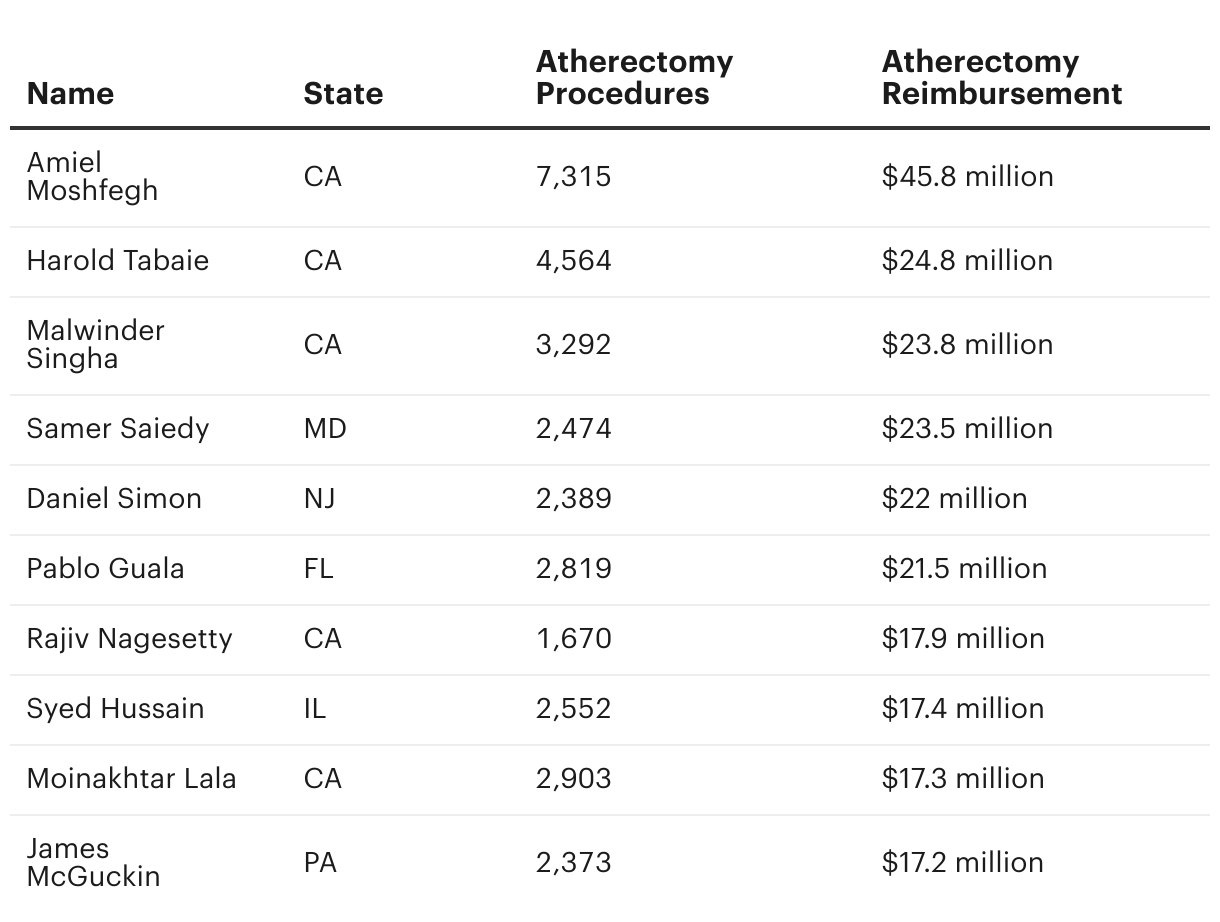
At the top of the list are three physicians from the greater Los Angeles area: Dr. Amiel Moshfegh with $45.8 million in Medicare reimbursement, Dr. Harold Tabaie with $24.8 million and Dr. Malwinder Singha with $23.8 million.
Doctors With Highest Medicare Reimbursement for Atherectomies From 2017 to 2021
Doctors With Highest Medicare Reimbursement for Atherectomies From 2017 to 2021

Relying on more detailed Medicare fee-for-service claims data analysis provided by CareSet, we calculated the number of patients who underwent a first-time atherectomy procedure during our study period when they appeared to have only had milder vascular disease based on a diagnosis of claudication.
Between 2019 through 2022, our analysis found that there were at least 121,000 patients who had first-time atherectomy procedures. Nearly 30,000 of these patients appeared to have more mild vascular disease, based on a diagnosis of claudication, according to the data, amounting to about 24.5%, or nearly 1 in 4 patients.
For about 170 doctors, half or more of their first-time atherectomy patients had only claudication as a diagnosis. And for nearly 780 doctors, a quarter or more of their first-time atherectomy patients had only claudication as a diagnosis. For more than 5,000 doctors, the number of claudication patients that had an atherectomy was too low to be reported, with fewer than 11 patients over four years.
Among high users of atherectomy, who conducted 200 or more procedures over four years, on average, about 15% of their patients appeared to have had more mild vascular disease based on a diagnosis of claudication.
Doctors Who Treated Most First-Time Atherectomy Patients With Milder Vascular Disease From 2019 to 2022
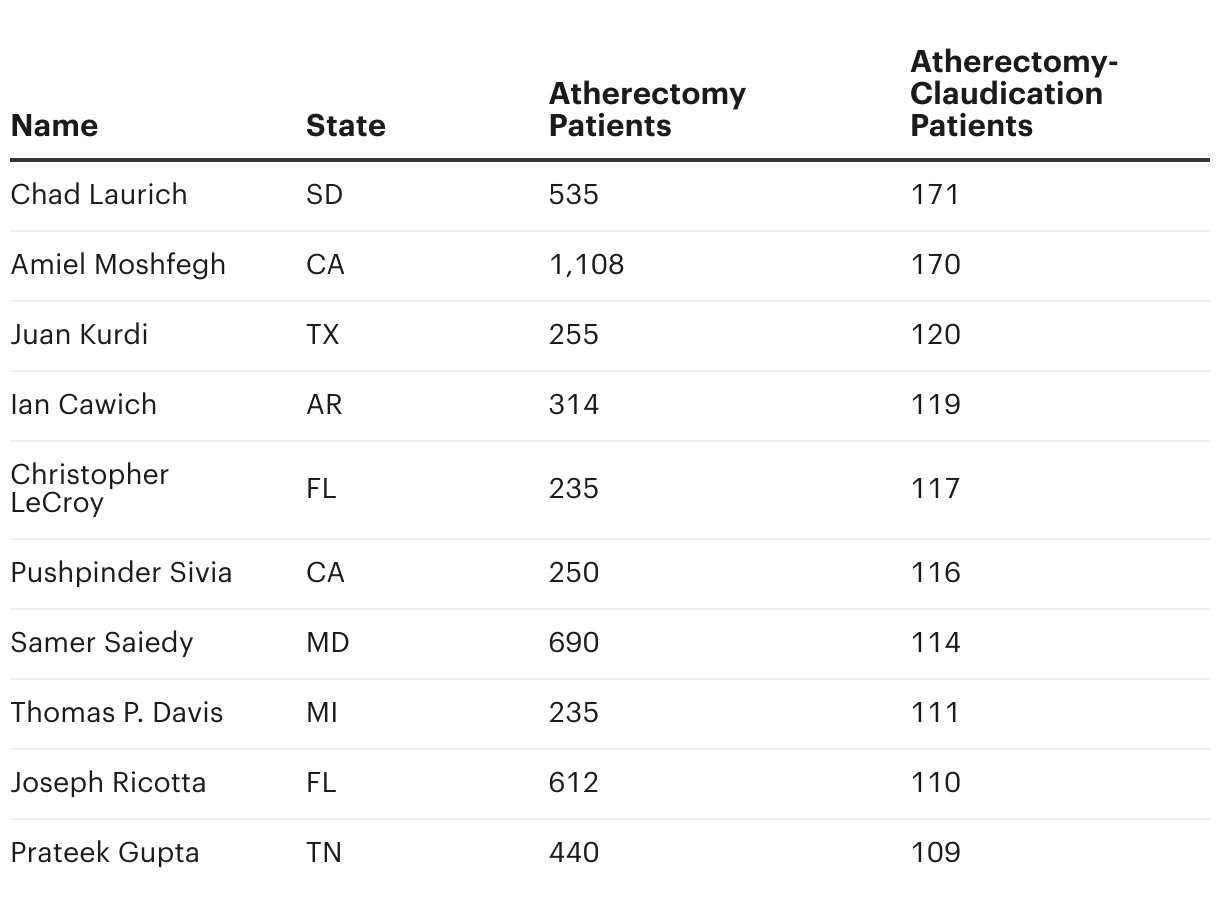
Doctors Who Treated Most First-Time Atherectomy Patients With Milder Vascular Disease From 2019 to 2022

Doctors Who Treated Largest Percentage of First-Time Atherectomy Patients With Milder Vascular Disease From 2019 to 2022
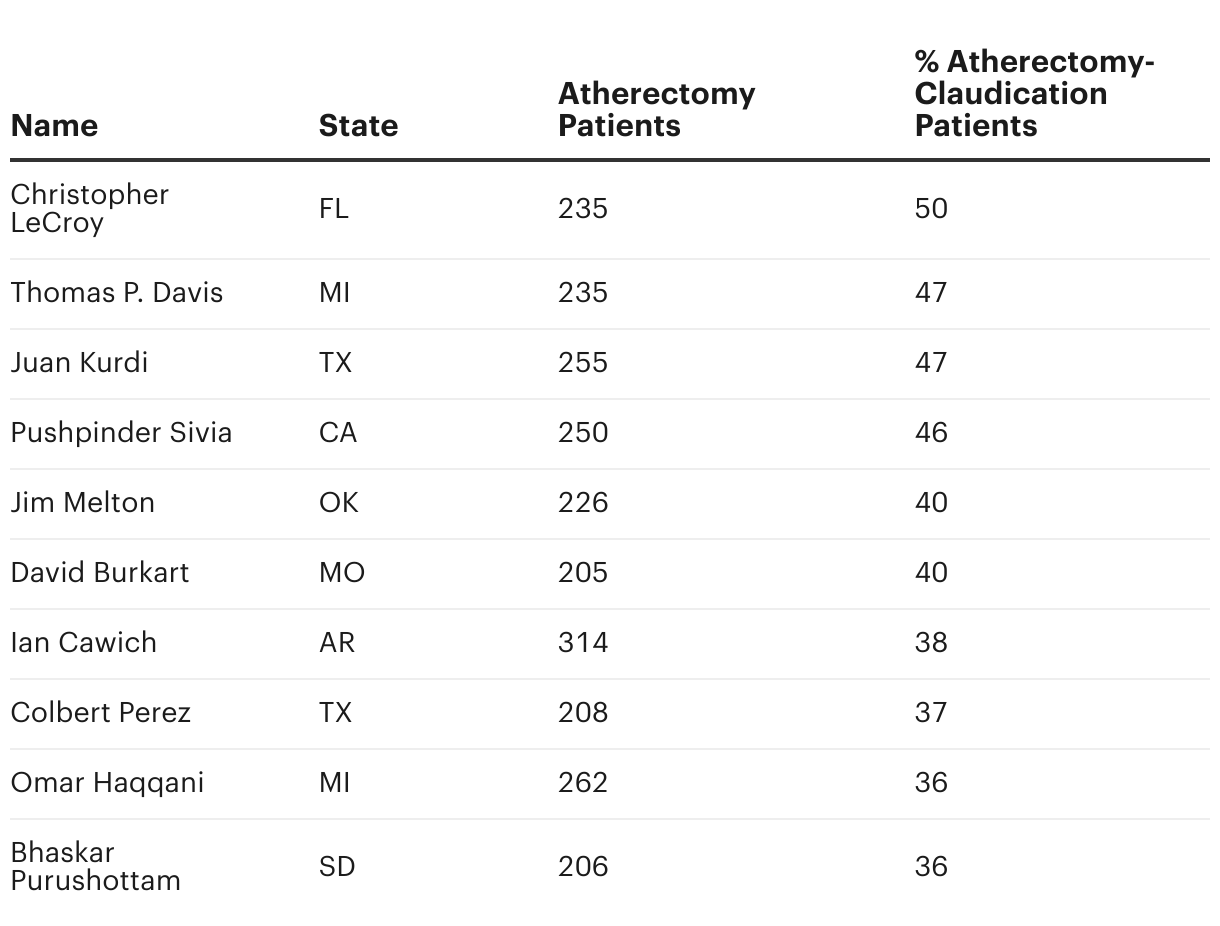
Doctors Who Treated Largest Percentage of First-Time Atherectomy Patients With Milder Vascular Disease From 2019 to 2022

While the data enables us to identify doctors that appear to have outlier treatment patterns, it does not allow us to determine the precise clinical reason why the doctors differ from peers or their motivation for conducting more procedures than other physicians. But researchers and experts told ProPublica that given the financial incentives to conduct atherectomy procedures in outpatient facilities, these patterns should raise alarms.
What Are the Limitations of Our Analysis?
Our analysis has some limitations. It relied on Medicare fee-for-service claims data, which is submitted by providers for financial purposes. While the data is supposed to be accurate, we cannot account for errors or inaccuracies — in particular, related to procedure or diagnosis codes — in what providers submit to Medicare. Despite the fact that electronic health record data is a richer resource, we did not use it as it’s not available at the scale required to conduct this study.
Medicare claims data only covers beneficiaries of the federal insurance program, and therefore we cannot make direct conclusions about beneficiaries with other insurance coverage. For patients with other insurance coverage, treatment patterns may look different. That said, it is estimated that more than 98% of American adults over the age of 65 are enrolled in Medicare, and about half of them appear in the fee-for-service data, which makes it one of the largest pools of health care information in the world.
Because Medicare claims data was submitted for billing purposes, it does not have complete clinical information on patient symptoms or disease severity. We do not have detailed information about arterial lesions, such as their exact locations, size or degree of occlusion, or clinical imaging, both of which might factor into a patient’s treatment plan. We also do not always know whether medication, exercise therapy or other less-invasive treatments were attempted before an invasive procedure, and if so, for how long. These kinds of programs are often not covered or tracked as part of the financial transaction.
Dr. Robert Tahara, president of the Outpatient Endovascular and Interventional Society, which represents doctors who treat vascular disease outside of hospitals and often in their own private practices, said Medicare’s claims data is not detailed enough to draw conclusions about doctor behavior. Tahara, who was not an outlier in our data, said that the data does not provide information on the stage of patients’ disease, their disease progression or whether medical therapy didn’t work for them — details that could provide a greater understanding of why a treatment was chosen. “For example, the patient’s claudication could be worsening and coming close to critical limb ischemia, but the claim could still include a code for intermittent claudication,” he wrote in an email.
We relied on a 12-month lookback to determine whether the atherectomy was a first-time procedure. If a patient received an atherectomy before 2018, it is possible that we have identified a follow-up procedure rather than their first-time intervention. However, this should not impact our findings of whether they received an atherectomy when their recent diagnosis was for claudication.
As part of the data use agreement, we are unable to display data for doctors with fewer than 11 patients because of privacy concerns.
How Did Doctors React to Our Data Analysis?
Several experts and doctors called our findings concerning. Dr. Marty Makary, a professor of surgery and health care quality researcher at Johns Hopkins University School of Medicine, has used similar Medicare claims data to research outlier practice patterns and said that our analysis reinforces his own findings. “It is validating concerns on the grounds that some physicians are responding to a perverse financial incentive,” he said. “The data suggest they may be doing procedures on people who don’t need them.”
Makary leads Global Appropriateness Measures, a consortium of physicians who use clinical wisdom and health care data to detect outlier patterns and discourage overuse. Outlier analyses are critical for improving health care, he said, as most physicians change the way they practice when they learn that they stand out. “Our general principle is that 83% of outliers reduce their pattern of overuse after they see where they stand on the bell curve,” he said.
But several private practice doctors, including some of the outlier physicians we identified in our analysis, rebuffed our analysis or took issue with the use of Medicare claims data.
ProPublica reached out to every doctor named in our story through multiple emails and phone calls, providing questions to the physicians, their clinics, hospitals or lawyers. The following doctors, their offices or lawyers did not respond to ProPublica’s questions for this story at the time of publication: David Burkart, Ian Cawich, Thomas P. Davis, Pablo Guala, Omar Haqqani, Syed Hussain, Juan Kurdi, Moinakhtar Lala, James McGuckin, Jim Melton, Rajiv Nagesetty, Daniel Simon, Pushpinder Sivia and Harold Tabaie. Dr. Bhaskar Purushottam and Monument Health, where he works, both declined to comment. Riverside Healthcare in Illinois, where Hussain has worked since September 2022, declined to comment on the doctor’s practice. Kurdi’s lawyer declined to comment.
Florida vascular surgeon Dr. Joseph Ricotta, the national medical director of vascular surgery and endovascular therapy at Tenet Healthcare, said he rarely intervenes on patients with claudication, unless they have severe lesions. “The overwhelming majority of claudicants obviously we don’t intervene on,” he said. “The majority are managed with medical therapy.” Medicare claims data does not provide detail on the severity of arterial lesions, he said.
Maryland vascular surgeon Dr. Samer Saiedy, who was an outlier in the data, echoed these concerns and said the data doesn’t include enough details to provide a full picture of why he may have treated a patient with an invasive procedure. At his practice, patients are only given the option of invasive procedures, he said, if they have severe pain and have already tried less aggressive approaches first.
“If you look at atherectomy only, and you narrow down, yes, I’ll be an outlier because I do a lot of claudicants for severe symptoms after we do the medical treatment,” he said. “They cannot walk through the pain, they’re already on blood thinners, they’re already on this and already on this. We’re going to do something.”
Tennessee physician Dr. Prateek Gupta also took issue with our analysis, which he called “incomplete,” stating in an email that he is not “an outlier when you analyze all of the necessary factors.” Our analysis, he said, attempts “to allege medically unnecessary treatment based upon one factor” and that “a professional medical opinion about medical necessity is based upon multiple factors, indicia of disease, prognosis, anticipated patient outcome, alternative treatment options, patient preference and others.” Claudication can sometimes be debilitating for patients, he said. “As a practice with protocols, we manage most claudicants conservatively with medical therapy,” he said. “Patients with severe claudication get offered endovascular or open surgical procedures based on their comorbidities and preference if medical therapy fails.”
Jessica Johnson, the chief operating officer of South Dakota’s Vascular & Interventional Specialists, where Dr. Chad Laurich works, did not respond to specific questions regarding ProPublica’s analysis but said that the vascular surgeon had an “unwavering dedication to advancing vascular surgery while prioritizing patient well-being.” The community has “experienced improved wound healing, saved limbs, improved quality of life and many lives saved,” she said. Laurich did not directly respond to ProPublica’s questions.
Cherlynn Hecker, the clinical director at Dr. Christopher LeCroy’s practice, said that he doesn’t conduct procedures on patients with mild disease unless they have lifestyle limiting pain and have already tried exercise and medication therapy first. “This endovascular work is preventing patients having bypasses or amputation,” she said. LeCroy did not directly respond to ProPublica’s emailed questions.
Some doctors said billing errors explained their high rates of intervention on claudication patients. Dr. Colbert Perez said that his practice, Caprock Cardiovascular Center & Cath Lab in Lubbock, Texas, had been marking their patients with incorrect diagnosis codes in Medicare billing claims for several years, which made its patient population appear to have milder disease. Perez said that he rarely intervenes on patients with mild disease and that his practice, which outsources its coding and billing to another company, was looking into the billing issue and was in contact with CMS for corrections and changes. Billing errors can occur, but CMS mandates that physicians “are responsible for ensuring that claims submitted” under their name are “true and correct.”
Some physicians said that Medicare reimbursement data is misleading. Saiedy, who has made about $23.5 million from Medicare in reimbursements for atherectomy procedures over five years, according to federal data, said the payments cover all clinic expenses and are not going to him directly. “You have to look at the overhead of the practice,” he said. “That includes nurses, anesthesia, leases for the equipment, rent.”
California interventional radiologist, Dr. Malwinder Singha, who received $23.8 million in Medicare reimbursements for atherectomy procedures over five years according to federal data, echoed Saiedy’s concerns. “It is devoted to running of the [office-based laboratory] and only a tiny fraction is earned by the operator,” he wrote in an email to ProPublica. “I have to pay my employees and expenses for all the supplies (wires, balloons, stents, atherectomy catheters, etc.), imaging equipment, [electronic medical records], facilities rent, etc.”
Read More


Singha also took issue with the use of claims data to identify clinical outliers. “It does not take into account the patient population I see and the severity of their disease,” he said. He added that outpatient facilities are safe, and their patients are satisfied with their care. “What I and my colleagues do is safe and effective,” he said. “There are hundreds of office-based labs who treat thousands and thousands of patients. The adverse event rate is minuscule.”
Dr. Amiel Moshfegh, who received over $45 million in Medicare reimbursements for atherectomy procedures over five years according to Medicare data — more than any other doctor in the country — said his atherectomy statistics reflect “the quality outcomes generated for patients and the confidence of referral sources in directing patients” to his practice. He did not answer ProPublica’s questions on his treatment of patients with claudication.
Interventional radiologist Dr. James McGuckin, who received $17.2 million in Medicare reimbursements for atherectomy procedures over five years according to Medicare data, treats “a significantly high-risk patient base” who are at-risk for amputation, said his attorney, David Heim in an email this past August.
Do You Have Experience With Peripheral Artery Disease? Have You Had a Procedure on Your Leg? Tell Us About It.
Some doctors may be overusing a procedure to clear out clogged arteries in legs, potentially leading to amputations. We need your help connecting with patients, including those who may not know they have had an atherectomy.
















